CLINICAL FINDINGS
- Knife-edge alveolar ridges
- Severe buccal-lingual ridge deficiencies
- Vertical and horizontal ridge collapse
- Missing anterior and posterior teeth
- Thin residual alveolar bone
- Buccal undercuts and contour deformities
- Deficient soft tissue architecture in esthetic zones
- Severe localized alveolar ridge resorption
- Insufficient vertical and horizontal ridge dimensions
- Buccal-lingual bone deficiencies
- Residual ridge width commonly 1–4 mm
- Significant osseous defects precluding implant placement
- Postoperative radiographs demonstrated successful graft incorporation and implant stability
Bone Grafting Challenges
- Autogenous grafts require second surgical donor sites
- Morbidity from iliac crest, ramus, symphysis, or tibial harvesting
- Bone graft resorption rates of 16–20%
- Technique sensitivity of ridge augmentation procedures
Advantages of Allogenic Block Grafts
- Avoid donor-site morbidity
- Reduced surgical invasiveness
- Predictable ridge width and height reconstruction
- Histologic evidence of active bone replacement and remodeling
- High graft survival rates (93%)
- Implant survival rate approximately 99%
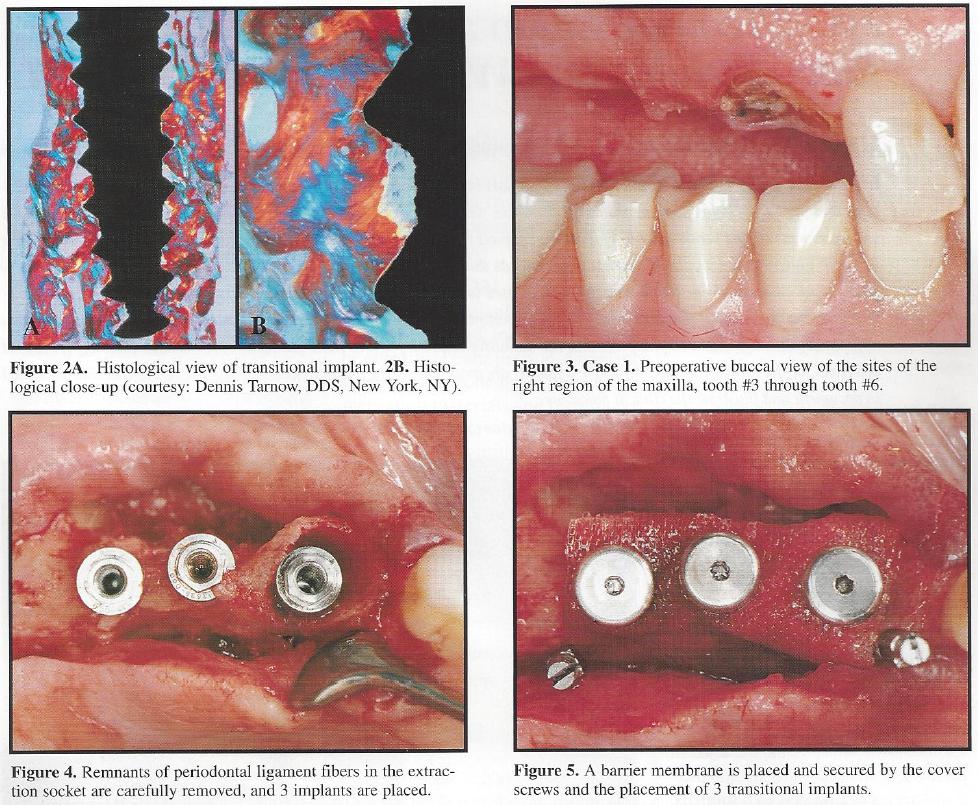
Transitional Implant Concepts
- Fixed temporization stabilizes grafted sites
- Prevents pressure on healing grafts
- Improves patient comfort and function during osseointegration
- Allows uninterrupted healing and soft tissue maintenance
Stem Cell Block Grafting
- Stem-cell infused allogenic blocks stimulate osseous regeneration
- Over 140,000 stem cells placed in grafted regions
- Improved buccal-lingual ridge reconstruction
- Reduced need for autogenous harvesting procedures
Surgical
TOPIC F - STEM CELL RIDGE AUGMENTATION
Missing teeth with inadequate bone volume for implant placement Severe ridge resorption and esthetic defects Difficulty restoring function and esthetics due to deficient alveolar contours Need for implant-supported rehabilitation